Rhinoplasty CASE STUDIES







Rhinoplasty
Rhinoplasty or nose job surgery in Orange County is designed to complement your facial features with a well-proportioned nose. Rhinoplasty surgery will improve your nose size and shape in order to achieve facial balance by altering the following:
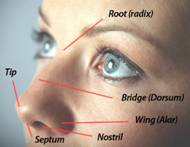
- Your nose width at the upper and middle (called the bridge) and the lower (tip) region.
- Your nose profile by lowering humps or filling depressions along the dorsum.
- Your nasal tip shape and position that may be enlarged or bulbous, drooping, upturned or hooked
- Your nostrils that are too large, wide, or upturned
- Your nasal asymmetry
If you desire any of these changes, you are encouraged to obtain a complimentary consultation with Dr. Paris. Specialist Orange County Rhinoplasty surgeon Mirzania has the experience and the artistic eye to create you an aesthetically pleasing nose with appropriate proportions that match your face.
Achieving a Natural Looking Nose
Expert Orange County Surgeon Mirzania, M.D., F.A.C.S., strives to give each patient a naturally appearing nose through rhinoplasty or nose job surgery. There has been a recent trend in cosmetic surgery to achieve aesthetically pleasing yet natural and non-operated-looking results.
Dr. Paris is well regarded for achieving natural results by working with the naturally occurring constructs of your nose and avoiding the introduction of foreign materials/distant grafts used by other surgeons only to camouflage underlying flaws resulting in an artificial and operated look.
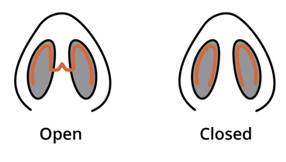
Dr. Paris specializes in altering naturally occurring features already present in your nose, even if they are shaped unfavorably. This results in you having a natural and non-surgical look to your new nose. Dr. Paris is able to achieve these results through both open and closed rhinoplasty techniques following years of experience and study in the field of Orange County rhinoplasty surgery.
Rhinoplasty Cost
The average cost of a closed rhinoplasty in Orange County is approximately $5,999. The average cost of open rhinoplasty surgery is $7,999. These costs are comprehensive and include surgeon and anesthesiologist fees as well as operating room costs. These prices are only an average and intended to give you a general guide to rhinoplasty costs. A consultation with our expert rhinoplasty surgeon will provide you an accurate cost of your rhinoplasty surgeon.
Rhinoplasty Cost
The benefit of open versus closed rhinoplasty depends on your desired nasal changes. Dr. Paris is considered an expert rhinoplasty surgeon of both approaches.
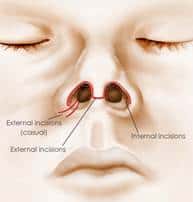
When considering undergoing nasal contouring Dr. Paris uses both approaches to rhinoplasty surgery in Orange County. The closed rhinoplasty technique utilizes two incisions that are made inside each of the nares in a semicircular pattern that is completely hidden.
These two incisions allow access to the upper and middle 2/3rd of the nose. This approach allows Dr. Paris to alter the nasal dorsum allowing narrowing the nasal bridge, elimination of the nasal hump, correction of a crooked nose and any dorsal irregularities.
However, the lower 1/3rd of the nose i.e. is not accessible. In contrast, the open rhinoplasty employs an incision across the columella, the fleshy bottom of the nose, and allows our expert rhinoplasty surgeon to access the entire nasal structures including the tip. Thus, the open rhinoplasty allows the correction of all of the nasal structures, including altering the nasal tip shape and position.
Please see the below diagram for the incision sites for open versus closed rhinoplasty
You might ask yourself why the open rhinoplasty approach is not employed on all rhinoplasty patients since it allows for contouring of the entire nose. The rationale for not utilizing this approach to all patients is multi-faceted. First, the open rhinoplasty requires a longer operative time. A longer operative time translates into increased rhinoplasty costs. Thus your decision to undergo closed versus open rhinoplasty should depend solely upon whether you wish to have your nasal tip shape or position altered.
Several questions will be covered Mirzania during your Orange County Rhinoplasty Consultation
Am I a good candidate for this procedure?
- What will be expected of me to get the best results?
- Where and how will you perform my procedure?
- What surgical technique is recommended for me?
- How long of a recovery period can I expect, and what kind of help will I need during my recovery?
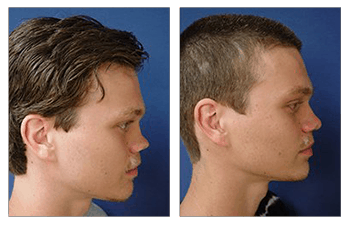
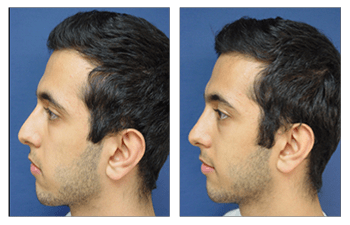
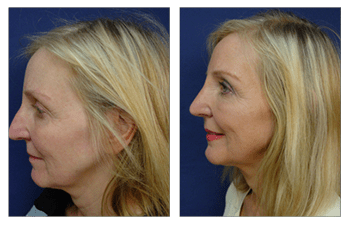
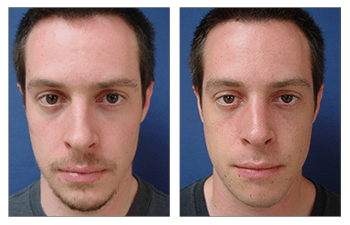
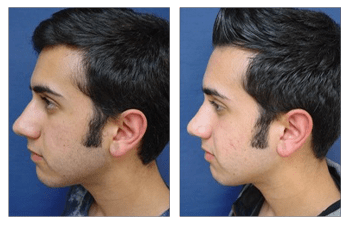
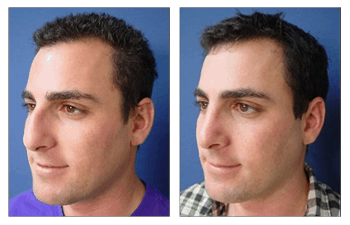
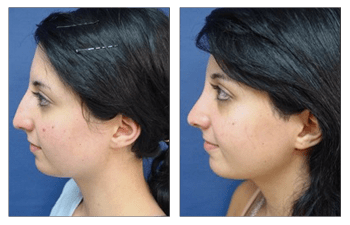
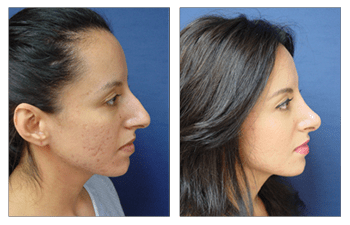
- Do you have before-and-after photos I can look at for this procedure and what results are reasonable for me?
If you live in Newport Beach or surrounding suburbs in Orange County, we encourage you to make a consultation with Dr. Paris to appreciate the improvements that nasal surgery could have for you.
Procedure
Improvement of nasal contour by various maneuvers including removing the nasal hump, narrowing the nasal base, and/or improving highlights of the nasal tip.
Length
Ranges between 1-2 hours (closed rhinoplasty) and up to 3 to 4 hours (open rhinoplasty) of operative time.
Anesthesia
General anesthesia is usually recommended, as the breaking of the nasal bones is required to eliminate a nasal hump and reduce the nasal base width.
Place of Treatment
At an otpatient surgical suite or hospital operating room.
Recovery
The recovery period for nasal surgery with a return to daily activities is usually 1 – 2 weeks. Patients are asked to forego physical activities and exercise for approximately 4 weeks until the nasal bones have completely fused and are stable.
Duration of Results
Patients who have undergone nasal surgery can expect aesthetically pleasing results for life. Early revisions are rare and are typically discouraged. Late revisions are needed in younger patients whose nose will continue to grow and evolve through life.