Top Rated in Orange County
Upper Eyelid
Upper Eyelid CASE STUDIES

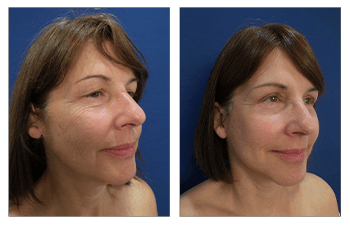






upper eyelid Surgery CASE STUDIES
Upper Eyelid
Recent discoveries involving upper eyelid aging changes have dictated advances in upper eyelid surgery. Upper eyelid surgery has traditionally involved removal of excess skin along the naturally occurring upper eyelid crease, as well as aggressive removal of herniated fat pockets which cause puffy eyelids. However, a close evaluation of the aging upper eyelid has demonstrated a natural tendency for the upper eyelid fat to melt away. As such, removal of fat pockets from the upper eyelid is generally avoided, and when performed, the fat is removed conservatively. In fact, patients who have previously undergone upper blepharoplasty will often complain of a gaunt or cachectic look as early as ten years following their surgery. These patients can regain appropriate fullness and rejuvenation by replacing the fat in their eyelids via fat grafting. This is a process wherein fat is harvested from another part of the body and then transferred in micropacules into areas that have lost fat.
Another advancement in upper eyelid surgery has involved refinements of upper eyelid incision line placement. Traditional incision lines were arched high, creating an operated or surprised look. Current standards dictate using lower incision lines that will appear more natural in their appearance. Although an arch-like incision is designed to parallel the natural curve of the eyelid margin, this arch is a gentle one. Using a lower and less arched incision line is most critical in male patients who are at risk of feminizing their eyes if the incision is not appropriately designed.
Procedure
Improvement in upper eyelid contour with the resolution of eyelid skin redundancy and upper eyelid bulge caused by droopy eyelid fat. Current upper eyelid surgery involves the removal of redundant upper eyelid skin and conservative resection of fat that is droopy.
Length
Ranges between 1/2 to 1 hour.
Anesthesia
Upper eyelid surgery can be performed under local anesthetic only, intravenous sedation, or general anesthesia.
Place of Treatment
Since upper eyelid surgery can be performed using local anesthesia only or with minimal intravenous sedation, it is not uncommon for your surgery to be performed even in an office setting.
Side Effects
1) The inability to close the eye is usually temporary and subsides over 1 week following surgery.
2) The redness of the incision lines may be noticeable for several weeks but is usually camouflaged as it falls in the naturally occurring upper eyelid crease.
3) Residual asymmetry of the lower eyelids may be present if asymmetry was pronounced preoperatively.
Risks
1) Deep vein thrombosis (DVT) may occur in the legs immediately following surgery when general anesthesia is used. DVT refers to the clotting off of leg veins which may result in compromised blood flow return from the legs; a more critical consequence may develop from this clot if it is dislodged and travels to the lungs causing pulmonary emboli. Fortunately, this risk is avoided by the use of pneumatic compression boots that minimize this complication.
2) Bleeding or small hematoma may occur and refers to the accumulation of blood in the early postoperative period which pools into a pocket. Since the skin of the eyelid is limited, hematomas must be drained immediately as any increased build-up of fluid may result in disruption of your incision line and/or increase pressure on the eye globe itself.
3) Infection: An infection can occur following lower eyelid surgery but is very rare. The eyelid tissue as is the facial skin is very well vascularized and not likely to get infected. In addition, lower eyelid patients are provided antibiotic eye drops which should suppress any potential bacterial growth.
4) Dry eyes: Dry eyes may develop as a result of changing pressures on the eyeball caused by the tightening of the overlying eyelid skin. The increase in pressure is believed to affect the eye lubrication and draining system (lacrimal system) which keep the moistened at all times. Patients who have a propensity for dry eyes preoperatively should be cautioned about developing this complication. Fortunately, as the eye accommodates to its new state, dry eyes tend to resolve over several months.
5) Visual compromise: Although this an extremely rare complication, it is conceivable that direct damage to the globe of the eye and/or the vascularity of the globe could occur resulting in blindness.
Recovery
The recovery period for upper eyelid surgery with a return to most daily activities is around 3 to 4 days. Patients will typically return to work within 1 week following surgery.
Duration of Results
Patients who have undergone upper eyelid surgery can expect aesthetically pleasing results for life. Early revisions are rare and are typically discouraged. Patients will notice turning back of the clock of approximately 15 years following upper eyelid surgery and will notice a natural resuming of the aging process.
FREQUENTLY ASKED QUESTIONS
What is the history of upper eyelid surgery?
The first upper eyelid was performed in 1890 by two physicians named De Mars and Marx. The first upper eyelid in the United States was performed by Dr. Kelly nearly a decade later. Over the last century upper eyelid techniques have continued to be refined.
Am I a good candidate for upper eyelid surgery?
In order to determine if you are a good candidate, your upper eyelid consultation will require evaluation of several items. First, the surgeon must assess degree of skin redundancy or flaccidity. This will determined the extent of the skin excision that will be required. In addition, the surgeon will evaluate the extent of excess and/or protruding fat that you have over the central and medial (close to the nose) eyelid regions. These fat pockets are located in specific locations in the eyelid referred to as the medial and lateral compartments. Secondly, your surgeon will ask you about any recent visual acuity changes, history of dry eyes, or double vision. If any of these conditions are present, then you will require a thorough work up by an ophthalmologist prior to considering upper eyelid surgery. Most patients demonstrating upper eyelid aging signs that result in a “tired” look are excellent candidates for this surgery. A few patients may demonstrate drooping of their lids due to poor muscle function which may be treated by upper eyelid surgery but does require more extensive surgery involving repairing the “lifting” muscle of the eyelid in addition to just removing redundant skin and fat.
What does upper eyelid surgery involve?
The upper eyelid procedure incorporates eliminating excess skin and conservative removal of protruding eyelid fat. Amount of upper eyelid skin removed is dependent on the degree of skin laxity. While waiting in the preoperative area and while the client is awake, the amount of redundant skin can be marked so that over resection of skin is avoided. Recent studies on aging have revealed a propensity for loss of overall fat volume in the face and eyes. These studies have prompted surgeons to be more conservative with removal of protruding eyelid fat. Many older clients who had more aggressive removal of fat are now returning to surgeon’s offices with a hollowed out appearance of their upper eyelid, termed the “gaunt” look. Fat pads in the upper eyelid are found in the central(middle) and medial(next to the nose) compartment. Today, conservative removal of fat is advocated and usually involves the medial fat pad only.
How do I plan my upper eyelid surgery?
On your initial visit, the surgeon will evaluate your health status, determine the amount of skin redundancy, and check your blood work. If you are a smoker, then you should quit for 1 month prior to upper eyelid surgery in order to allow your body adequate time to rid itself of any residual nicotine. Nicotine in your system results in shutting off of small blood vessels which carry nutrients to the skin, which will hinder your healing and possibly compromise your surgical incision healing. If you have been experience recent visual acuity changes, you should have your eyes checked in order to have a baseline vision test prior to surgery.
How do I prepare for upper eyelid surgery?
Since your surgery may be performed with local anesthetic solution and/or minimal intravenous sedation, you must make minimal precautions prior to surgery. First, you don’t have to avoid eating and drinking after midnight on the day before surgery. Since, you will be administered minimal sedation if any at all, you will have a quick recovery with minimal grogginess. Most patients comment on the ease of their postoperative recovery requiring minimal pain medications. However, due to localized swelling of the upper eyelid tissue, patients should have a friend or spouse look over them and drive them from the office as they will have obscured vision for the first 24 hours.
What results can I expect after upper eyelid surgery?
Following upper eyelid surgery, patients can expect a youthful upper eyelid contour with a well hidden surgical incision line. You will be amused by friends and family complimenting you on looking well rested and asking you if you have done anything. Your aesthetically improved results will last you several decades. On rare occasions, patients may request a touch up but only 20 to 30 years following surgery.
Where will my upper eyelid surgery be performed?
Since eye surgery can be performed using local anesthesia only or with minimal intravenous sedation, it is not uncommon for your surgery to be performed even in an office setting. Even when performed in the office, patients must be fully monitored and cared for by appropriate nursing staff. Patients may also request to have their surgery performed under general anesthesia which would necessitate their surgery to be performed in an office based operating room, surgery center, or hospital setting. It is of utmost importance for patients to make sure that the office based operating rooms have been accredited by a surgical accreditation body such as AAAASF.
What type of anesthesia will be used for my upper eyelid surgery?
Upper eyelid surgery can be performed under local anesthetic only, intravenous sedation, or general anesthesia. General anesthesia is recommended when synchronous surgeries are being performed such as a brow lift or facelift.
What should I expect after upper eyelid surgery?
When you wake up from your surgery, expect to find your visual capacity limited as your eyelids will be swollen and your vision blurry secondary to ocular lubricant that is placed in your eyes. You will notice minimal pain which will be well controlled with pain medications. You will need a caretaker for the first 24 hours as your eyelids will be swollen and you will have some difficulty maneuvering in the house; however, most patients feel that they are independent as early as the day following surgery. Expect your sutures to be removed within one week at which time you will find complete resolution of eyelid swelling and bruising.
When will I be able to return to work following upper eyelid surgery?
For patients who undergo a standard upper eyelid surgery, expect to return to work no later than 10 days following surgery. If your job does not require direct consumer interaction you may return to work as early as 4 days following surgery. You will have tiny clear sutures that will be removed at one week following surgery.
Are there any side effects associated with upper eyelid surgery?
There are several side effects that have been associated with upper eyelid surgery and these include:
a) Inability to close eyes (lagophthalmos) is a temporary condition that is common over the early period following surgery. Patients may note quick resolution of this difficulty when it is caused by paralyzed muscles that will recover once the local anesthetic wears out in a few hours. Minimal lagophthalmos may be present and will resolve over one week. Even if too much skin has been resected, the brows will compensate by drooping down to accommodate tightness in skin until the skin stretches on its own over the first month.
b) Redness of incision lines may persist while the incision line is healing over the first month following surgery. This is expected following surgery which involves placement of surgical incision lines. Fortunately, the incision lines are placed in the naturally occurring crease of the upper eyelid termed the supratarsal crease and are not readily visible.
c) Asymmetry of the eyelids may be present postoperatively especially when there is asymmetry present preoperatively. When significant asymmetry is present, patients should expect considerable improvement in symmetry as the surgeon makes all attempts to correct any residual asymmetry. As such, patients should realize that upper eyelids are not always identical and minimal asymmetry may be present.
Are there any risks associated with upper eyelid surgery?
a) Deep vein thrombosis (DVT) may occur in the legs immediately following surgery when general anesthesia is used. DVT refers to the clotting off of leg veins which may result in compromised blood flow return from the legs; a more critical consequence may develop from this clot if it is dislodged and travels to the lungs causing a pulmonary emboli. Fortunately, this risk is not commonly a concern as most upper eyelid surgeries are performed under local anesthetic and/or intravenous sedation alone.
b) Bleeding or small hematoma may occur and refers to the accumulation of blood in the early postoperative period which pools into a pocket. Since the skin of the eyelid is limited, hematomas must be drained immediately as any increased build up of fluid may result in disruption of your incision line and/or increase pressure on the eye itself.
c) Infection: An infection can occur following upper eyelid surgery but is very rare. The eyelid tissue as is the facial skin is very well vascularized and not likely to get infected. In addition, upper eyelid patients are provided antibiotic eyedrops which should suppress any bacterial growth.
d) Dry eyes: Dry eyes may develop as a result of changing pressures on the eyeball caused by the tightening of the overlying eyelid skin. The increase in pressure is believed to affect the eye lubrication and draining system (lacrimal system) which keep the moistened at all times. Patients who have a propensity for dry eyes preoperatively should be cautioned about developing this risk Fortunately, as the eye accommodates to its new state, dry eyes tend to resolve over several months.
e) Visual compromise: Although this an extremely rare complication, it is conceivable that direct damage to the globe of the eye and/or the vascularity of the globe could occur resulting in blindness.
PATIENT-SPECIFIC QUESTIONS
What does upper eyelid surgery involve?
The upper eyelid procedure incorporates eliminating excess skin and conservative removal of protruding eyelid fat. Amount of upper eyelid skin removed is dependent on the degree of skin laxity. While waiting in the preoperative area and while the client is awake, the amount of redundant skin can be marked so that over resection of skin is avoided. Recent studies on aging have revealed a propensity for loss of overall fat volume in the face and eyes. These studies have prompted surgeons to be more conservative with removal of protruding eyelid fat. Many older clients who had more aggressive removal of fat are now returning to surgeon’s offices with a hollowed out appearance of their upper eyelid, termed the “gaunt” look. Fat pads in the upper eyelid are found in the central(middle) and medial(next to the nose) compartment. Today, conservative removal of fat is advocated and usually involves the medial fat pad only.
How long do I have to take off of work for upper eyelid surgery?
The traditional upper eyelid involves removal of upper eyelid skin and minimal fat pad and is considered minimally invasive. Subsequently recovery is considered short and most patients are able to return to work within two to three days. Patients may elect to avoid important social engagements as small, clear sutures are removed at one week following surgery.
If I am planning facelift surgery can I be considered for an upper eyelid surgery?
Patients undergoing facelift surgery will realize a more youthful facial and neck contour. If the upper eyelids demonstrate signs of aging, then patients may find a discontinuity of their youthful face and neck following facelift surgery when compared to their aged upper eyelid contour. Patients are encouraged to consider upper eyelid surgery at the time of their facelift surgery if upper eyelid aging signs are present.
How does a forehead lift effect the upper eyelid contour?
Patients considering upper eyelid surgery should have a thorough evaluation of their brows. A lowered brow position will increase the degree of upper eyelid skin present. In contrast, surgery to lift the eyebrows, i.e. forehead lift, results in reducing the redundant upper eyelid skin. As a result, patients who undergo forehead and eyelid surgery synchronously, will have their eyebrows lifted prior to their upper eyelid surgery. This will then result in more conservative resection of the upper eyelid skin.
Will I have difficulty closing my eyes following upper eyelid surgery?
Temporary tightness of the upper eyelid skin is not uncommon. If patients experience tightness they will notice relaxation of their upper eyelid skins and complete closure within one week. In the early period, it may be prudent to place eye lubrication into the eyes in order to prevent scleral abrasions.
Where is my upper eyelid incision made?
Upper eyelid surgery requires excision of redundant upper eyelid skin. Excision lines are placed strategically so that the final surgical incision line will fall in the natural upper eyelid crease (termed the supratarsal crease). This allows for improvement of upper eyelid contour using a nearly invisible surgical incision line.
If I have thyroid disease can I still be considered for lower eyelid surgery?
Patients who have thyroid disease often present with enlarged eyeballs, medically termed proptosis. Patients with enlarged eyeballs have to be examined thoroughly preoperatively as they have an increased risk of developing an undesirable “pulled look” of their lower eyelid following lower eyelid surgery (termed ectropion). These patients may require a lower lid tacking procedure to supplement the routine lower eyelid surgery. Consultation with a board certified plastic surgeon is necessary to determined what maneuvers will be required intraoperatively to ensure an aesthetically optimum result.
If I am planning to have a facelift surgery can I be considered for a lower eyelid surgery?
If you are planning to undergo facelift surgery, you should be considered for having your lower eyelid surgery performed at the same time. Although facelift surgery utilizing the extended “high” SMAS facelift technique will result in removal of some lower eyelid hollow, often a lower eyelid surgery is also beneficial to remove redundant skin that may become even more apparent following facelift surgery.
Will I have any numbness following lower eyelid surgery?
Numbness of the lower eyelid skin following lower eyelid surgery is uncommon and usually temporary. Numbness immediately following surgery is secondary to postoperative swelling that is expected and which will resolve over the first several weeks.
Will my lower eyelid hollow be improved following lower eyelid surgery?
Patients who present desiring lower eyelid surgery often complain of redundant skin, bulging of the upper aspect of the lower eyelid skin, and hollow of the lower aspect of the lower eyelid skin.
What lower eyelid changes can I expect to change with lower eyelid surgery?
Lower eyelid surgery will remove bagginess, fatty protrusions, upper face hollowness, lax hanging skin, and improve overall lower eyelid contour.
What is Blepharochalasis?
Blepharochalasis is a rare inherited disorder that appears in childhood; children will notice repetitive episodes of eyelid swelling that eventually leads to loosening of eyelid muscles that help lift the upper eyelid (levator muscle). Eventually, these children will notice drooping of their eyelids.
What is Dermatochalasis?
Dermatochalasis refers to the stretching and redundancy of eyelid skin associated with aging changes.
What is Steatoblepharon?
Steatoblepharon is the medical term for herniated eyelid fat that protrudes under the eyelid skin and results in puffiness of the lower eyelids.
What is eyelid ptosis?
Eyelid ptosis refers to the drooping of the upper eyelid margin that is caused by stretched out or weakened muscle of the eye which helps lift the eyelid (levator muscle). This condition must be detected by your plastic surgeon prior to surgery as it will require tightening of your muscles in addition to the removal of the redundant skin and protruding fat pad.
How many fat compartments exist in the eyelids?
There are two fat compartments in the upper eyelid and three in the lower lid. If performed by non-trained physicians, the lacrimal gland located over the lateral aspect of the outer aspect of the eyelid may be confused as a fat compartment. Inadvertent injury to the lacrimal gland will result in dry eye syndrome.
How can someone go blind during eyelid surgery?
Although this complication is rare and devastating, it is observed following bleeding into the orbital socket likely caused by bleeding from a blood vessel around the eyelid fat compartments. Bleeding in this compartment is termed retrobulbar hemorrhage and may lead to collapse of the vessels that feed the eye globe if sufficient pressure accumulates in this space. Risk factors include high blood pressure or poor blood clotting capacity. If caught early, then release of the eyelid incisions and possible release of the lateral aspect of the eyelid margin (cantholysis), and infusion of a diuretic are necessary to prevent permanent damage.
Are there different causes for upper eyelid droop (ptosis)?
Several causes for upper eyelid droop exist and have been characterized as:
1) Myogenic (dysmyogenic) ptosis: most common congenital type, due to faulty development of the eyelid muscle that pulls the eyelid up (levator muscle).
2) Neurogenic ptosis: results from faulty innervation of upper eyelid lid retractors; ptosis is profound with complete interruption of innervation to levator muscle.
3) Mechanical or traumatic ptosis: results from any traumatic injury that interferes with levator muscle or its innervation;
What is postsurgical lagophthalmos?
This refers to the inability to close eyelids completely or to cover the globe adequately. It is common postoperatively due to swelling of the eyelid following surgery. If it does not resolve over the first several weeks it can be caused by over-resection of the upper eyelid redundant skin. Patients are provided artificial tears and/or lubricating eye ointment for routine surgical aftercare while this condition resolves.
What creates the natural upper eyelid crease?
The natural upper eyelid crease is called the supratarsal fold or crease. This crease occurs just above the upper border of a stiff structure called the tarsus. The tarsus provides structural integrity to the lower aspect of the upper eyelid so that it has stiffness and so that it does not flop around. This crease is created by the extension of the eyelid lifting muscle, called the levator, as it attaches to the skin.
What is the double eyelid operation?
This operation is often requested by patients of Asian ancestry who lack a supratarsal fold, the naturally occurring crease of the upper eyelid. This occurs because the eye lifting muscle, the levator, has either lost its attachments to the skin or the attachments are lower on the eyelid over the tarsus, the stiff portion of the lower aspect of the upper eyelid, thus not allowing for the naturally occurring crease to occur or do not have the fold bilaterally; When the fold then is present, this creates two aesthetically pleasing segments to the upper eyelid referred to as the double eyelid. which is considered aesthetically normal. The double eyelid operation uses standard upper eyelid surgery techniques with the addition of re-establishing the levator connection to the upper eyelid skin.
Can children get baggy upper eyelids?
There exists a rare inherited disorder in children, called Blepharochalasis, which results in baggy upper eyelids. Children develop repetitive episodes of eyelid swelling that eventually stretches out all the tissues of the eyelid including, the skin, muscle, and structurally supporting tendons. These children often need a more complex reconstructive upper eyelid surgery.