WANT THE CONFIDENCE THAT COMES WITH
KNOWING YOU LOOK YOUR BEST?

Closed Rhinoplaty CASE STUDIES


Closed Rhinoplasty
Rhinoplasty Approaches - Closed versus Open Mirzania M.D.
Two approaches are available for nasal contouring and these include the closed versus open rhinoplasty approach. The closed rhinoplasty approach requires two separate incisions that are made inside each of the nares in a semicircular pattern which are placed at the junction of the middle and lower 1/3rd of the nose (called the inter cartilaginous incision).
These two incisions allow access to the upper and middle 2/3rd of the nose. As such, the nasal tip; or lower 1/3rd of the nose, its not accessible and not alterable by virtue of this incision placement.
In contrast, open rhinoplasty utilizes a modified form of the closed rhinoplasty incisions (marginal incisions) which are then connected across the lower aspect of the columella. By connecting these two incisions, the entire nasal skin envelope can be elevated and the infrastructure of all three components of the nose is visualized and alterable.
The open rhinoplasty provides full access to the entire nasal infrastructure and most importantly including the nasal tip.

So why is the open rhinoplasty approach not utilized for all prospective rhinoplasty patients since it allows for contouring of the entire nose? The reason for not utilizing this approach for all patients is multifold.
First of all, the open rhinoplasty requires substantially longer operative times by virtue of requiring not only increased dissection and closure times but also more extensive structural supporting maneuvers.
Longer operative times translate to increased financial constraints on patients since surgical prices are depending on operative lengths. As alluded to above, placing an incision in the columella and dissecting the nasal tip structures and subsequent repair of the columellar incision will affect nasal tip projection.
During the healing of the columella incision line, the tip structures are required during all open rhinoplasties to avoid nasal tip collapse does introduce unnecessary risk to nasal surgery that is avoided by the closed rhinoplasty approach.
In contrast, when the nasal tip requires alteration and improvement in highlights, then the open rhinoplasty is far superior to the closed rhinoplasty technique.

Nasal Hump Mirzania M.D.
The most commonly sought out nasal contouring procedure involves lowering and/or narrowing of the nasal dorsal bridge (top of the dorsum) or nasal dorsal base (bottom of the dorsum) and eliminating of the nasal dorsal hump (Figure 18).
The dorsal hump is the undesirable prominence that is frequently seen on the dorsum of the nose and is comprised of two components.:
- The upper part of this hump is made up of prominent nasal bones located over the upper 1/3rd of the nose
- The lower part of the dorsal hump is made up of a prominent upper lateral cartilage and septum located over the middle 1/3rd of the nose
The treatment of an isolated wide and prominent dorsal hump only requires a closed rhinoplasty, as this internal nares incision provides access to both of these regions as described prior.
(Figure 17)
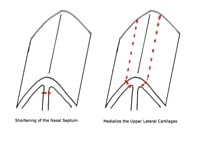
First, the lower part of the hump is addressed. This procedure requires isolation of the fusion point of the upper lateral cartilage and the dorsal septum that creates a canopy, this fusion point is released bilaterally.
This maneuver then allows for differential lowering and/or narrowing of the dorsal hump. To only lower the dorsal hump height, the dorsal septum is trimmed down and to only narrow the dorsal width the medial aspect of the upper lateral cartilages is trimmed which allows the upper lateral cartilages to medialize (Figure 17).
If both lowering and narrowing of the dorsal hump are desired, then both structures are trimmed. Following the reduction of the cartilaginous component of the hump, the bony component of the hump is addressed.
(Figure 18)
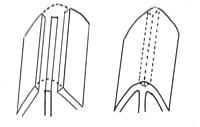
First, the roof of the hump is lowered to lower the dorsal bony height and resulting upper part of the hump; this is done by a combination of a medial osteotome and/or rasp which is used to literally remove the top of the nasal dorsal roof.
This maneuver completes the reduction of the dorsal hump height, but results in a disconnect of the bony dome often referred to as an open roof deformity (Figure 18). Thus, the lateral base of the nasal bones where they rise off of the maxillary bony foundation requires release by use of a lateral osteotome
This maneuver allows the nasal bones to be transposed medially thus re-establishing the bony roof as well as to narrow the nasal bony dorsum bridge and base. Less frequently, patients may have some asymmetry of the actual dorsum in addition to a hump.
Minor asymmetries are correctable by adjusting the degree of nasal bone medialization during the above release. For example, if one side is narrower than the other, then naturally the narrower side does not have to be brought I as much.
Following release and repositioning of the nasal bones, the bones are held in place to fuse by use of an external splint which is kept in place as a cast for one week.
Others might have nasal dorsum asymmetries related to having a crooked/or twisted dorsum. Minor crooked/twisted noses can be set back to the center by differential medialization of the nasal bones as above, and differential trimming of the upper lateral cartilages and with the use of graphs between the upper lateral cartilage and septum.
When sewing in the graphs (named spreader graphs), it is possible to further influence the shape of the nasal dorsum. For example, if the nose is crooked and leaning to the right, one can use the left upper lateral cartilage and sewn in graphs to act as cantilevers and to pull over the septum to the middle.
Frequently Asked Questions:
The doyle splint is intended to keep the nose aligned and to keep the internal mucosal surfaces away from each other until they are healed. We keep the splints in place for one week only.
Unfortunately, to correct tip shape you will require a revision open tip rhinoplasty. If the tip cartilages were not positioned appropriately in the tip, you may look like a bird; also too much removed from the lateral supralar region causing the pinching which will require cartilage grafts.
A bump after rhinoplasty is common and due to the sawdust of bone that reforms a bony prominence; this can be removed using a rasp in the office to save you money on the revision.
Patient-Specific Questions:
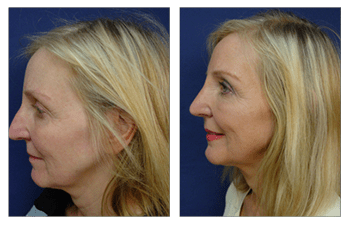
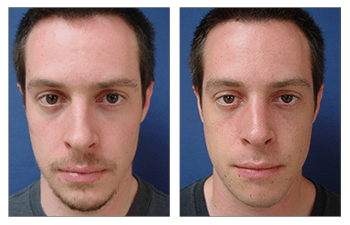
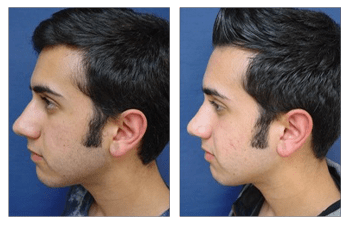
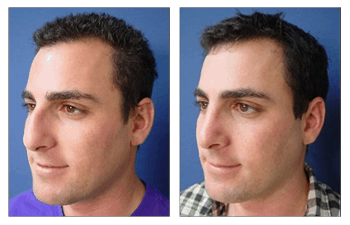
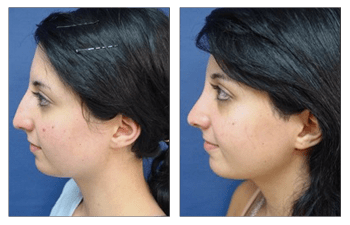
Closed rhinoplasty will result in narrowing of your nasal bridge and base and elimination of nasal hump. it can be done in less than an hour and is very affordable. A skype or facetime consultation with a nasal specialist can help you appreciate the difference that a closed rhinoplasty will make for you and help you with getting fee estimates
Residual nasal hump may develop after closed rhinoplasty and I feel is caused by residual bony dust that remains following rasping. This can be corrected in the office with local by performing a re-rasping.
All you need to do to your nose is to take the dorsum down slightly so that it has a slight concave rather than convex contour. this can be done in one hour using a closed rhinoplasty approach; this will save you lots of money !