WANT THE CONFIDENCE THAT COMES WITH
KNOWING YOU LOOK YOUR BEST?

Author: Paris Sabo MD
Fellowship Trained, Cosmetic Surgeon



Arm Lift Surgery
Arm lift surgery requires both the elimination of skin redundancy as well as the removal of fat excess. Arm lift surgery, i.e. Brachioplasty, is a common procedure performed in patients who have undergone significant weight loss, such as following gastric bypass surgery.
Arm lift patients will typically complain of "bat wings" along the underside of their upper arms that flop out of their blouses or shirts. These patients will often avoid wearing short sleeve shirts because the appearance of their arms makes them self-conscious of the Skin. Arm lift surgery involves liposuctioning of excess fat first followed by excision of skin redundancy.
Brachioplasty that is intended for post-bariatric patients has been modified from traditional techniques to address the severe skin redundancy that follows large weight loss.
Traditional Brachioplasty excision lines were designed to fit in your armpit which only allowed for the elimination of minimal skin redundancy but with a hidden excision line; these excision line designs were determined to be inadequate for removal of more extensive skin redundancies noted in large weight loss patients.
As such, these excision lines were modified to lie along the length of the arm and directly over areas of skin redundancy. Although this excision line runs along the entire length of your upper arm, it is placed strategically at the bottom of the arm so that when your arms are tucked down on your sides, the incision lines are hidden.
Today, these modified longitudinally oriented Brachioplasty excision lines have become the gold standard procedure that allows for maximum removal of redundant skin. Moreover, universal liposuction is first performed not only to remove any excess fat but also to hydro-dissect some of the more vital structures from being damaged during the later skin excision portion of the surgery.
Vital structures such as the basilic and cephalic veins as well as the median sensory nerve are protected by virtue of being dissected away from the excision plane.
By utilizing hydrodissection of the soft tissues and protecting the above structures, two common side effects of Brachioplasty surgery are avoided and these include:
- Prolonged arm swelling
- Arm insensitivity
Following your initial consultation, Dr. Paris will customize your Brachioplasty surgery to limit your incision line length as well as visibility yet maximize undesirable upper arm skin redundancy. Dr. Paris will also evaluate your fat excess to guide your simultaneous liposuction, arm fat surgery.
Recently, an alternative to traditional arm lift surgery involving skin excision has been developed and been coined as a minimally invasive Brachioplasty. Arm fat surgery is still utilized to first remove the excess fat using liposuction.
However, Vaser liposuction is specifically used since it provides the advantage of removing the fat from the most superficial layer in the skin in addition to the deep layer. This is in contrast to traditional liposuction that only removes the deep layer of fat.
It is the removal of this fat layer that allows for the reduction in skin redundancy using a newly developed technology, coined Renuvion subdermal coagulation. Removal of the superficial fat underlying the dermis allows for the application of Renuvion technology to tighten the skin without the need for skin excision.
Renuvion technology utilizes helium activated radiofrequency to heat and subsequently shorten collagen fibrils on the undersurface of the skin dermis. Collagen tightening occurs instantly as seen by immediate skin tightening observed in the operating room.
When combining arm fat surgery using Vaser liposuction with Renuvion technology, high definition arm contouring is accomplished even in patients with moderate skin redundancy. This alternative to Brachioplasty has expanded our client population desiring arm lift surgery. The client population desiring arm lift surgery now includes younger patients in their thirties and forties who do not want the stigma of an excision line since they are more active and are apt to wear clothing that shows their upper arms.
In addition, we are observing patients in their 70s and 80s that are wishing to eliminate their grandma bat wings. The older patient clients have always been desiring to have their grandma arms rejuvenated but they have feared the healing of a more invasive traditional excisional surgery as well as wanting to avoid general anesthesia. The most important advantage of minimally invasive Brachioplasty might the fact that it can be performed without general anesthesia. To see if you are a candidate for minimally invasive Brachioplasty, a Skype or Facetime consultation is recommended.
Arm lift recovery is typically considered very tolerable. Patients will find themselves wrapped with compression dressings that extend down from their armpits to their wrists. The reason for a full-length arm dressing is to avoid arm swelling that can develop over the distal, lower arm if dressings are not extended down the full length of the arm, called the tourniquet effect. Patients are asked to maintain their arm dressings for a minimum of two weeks until initial swelling resolves.
Patients are allowed to return to regular daily activities no more than 2 weeks following surgery and to return to full physical activity no more than one month following surgery. Patients typically find Brachioplasty surgery comfortable and the pain tolerable. Patients undergoing minimally invasive Brachioplasty, i.e. scarless arm lift, will typically require more frequent follow up over the first 10 days following surgery which includes 5 sessions of aggressive lymphatic massage but will find their overall recovery even less strenuous than traditional Brachioplasty. This is because they will avoid having to heal long surgical excision lines.
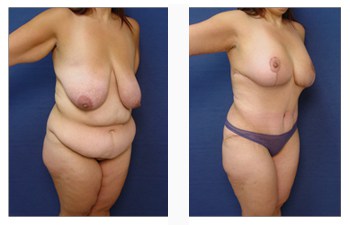
The surgical excision line has historically been the major disadvantage of traditional arm lift surgery. This is because even though the incision lines do heal well, they do demonstrate a prolonged six months to the one-year healing period before they are maximally faded. In contrast, patients with moderate to severe skin redundancy undergoing minimally invasive Brachioplasty may observe some skin wrinkling that tends to dissipate over the first four to six months. Dr. Paris encourages patients interested in arm lift surgery to view the Brachioplasty before and after photographs to appreciate the nuances of both traditional and minimally invasive arm lifts prior to making their preferred arm lift technique.
Frequently Asked Questions:
What does brachioplasty surgery involve?
Brachioplasty surgery involves the removal of redundant skin and residual fat that may have resulted following weight loss over the upper arms.
Brachioplasty surgery requires direct excision of redundant skin and liposuction of the residual fat located over the upper arms. The resulting incision is repaired using a layered plastic surgery closure that minimizes tension on the closure. Patients undergoing brachioplasty will enjoy a lifelong of sleek and youthful appearing upper arms.
Am I a good candidate for brachioplasty surgery?
You are a good candidate for brachioplasty surgery if you have noticed flaps of skin that are hanging off of your upper arms like bat wings. These flaps of upper arm skin can be unsightly to the point of avoiding wearing short sleeve shirts.
How do I plan my brachioplasty surgery?
On your initial visit, Dr. Mowlav will evaluate your health status, determine the amount of skin redundancy and residual fat, and show you a customized excision line; You will that have your blood checked.
Expect to have iron and Vitamin B12/Folate deficiencies. The iron deficiency will result in a low blood count, which must be corrected before surgery. The correction of the low blood count will take at least 1 month and require taking daily iron pills.
If you are a smoker, then you should quit for 1 month prior to brachioplasty surgery in order to allow your body adequate time to rid itself of any residual nicotine. Nicotine in your system results in shutting off of small blood vessels that carry nutrients to the skin; this event could be catastrophic in brachioplasty surgery resulting in extensive wounds requiring months to heal.
How do I prepare for brachioplasty surgery?
Since your brachioplasty surgery will require general anesthesia, you must take several precautions prior to surgery. First, you will have to avoid eating and drinking after midnight on the day before surgery. This precaution ensures that your stomach is clear of digested foods that could potentially be aspirated and contaminate your lungs during the induction of anesthesia.
Since you will have anesthetic medications administered throughout the case, you will remain groggy for some time and will require a ride to and from the surgery center if you elect not to commit to an overnight stay on the premises. You should choose a caretaker who is conscientious and who can spend the first night with you.
What results can I expect after brachioplasty surgery?
Overall, brachioplasty patients should be commended for their due diligence in losing their excess weight. By providing these patients with a final skin reduction procedure for their upper arms, we are able to obtain for you the contoured upper arms that you have dreamed of.
Patients are extremely satisfied with their surgery and their desire to wear short-sleeved shirts. By providing a thorough preoperative workup, safe intraoperative course, and frequent postoperative visits, patients should expect a speedy recovery and return to a more aesthetically pleasing upper arm contour and enjoy more freedom with their choice in clothes.
Where will my post brachioplasty surgery be performed?
Since your brachioplasty surgery will require general anesthesia, it must be performed in an operating room that is part of an outpatient surgery center or in an in-house office-based operating room, but it is of utmost importance for patients to make sure that the office facility has been accredited by a surgical accreditation body such as AAAASF.
What type of anesthesia will be used for my brachioplasty surgery?
Since your brachioplasty surgery requires the removal of moderate amounts of skin in an area of the arm that is very sensitive, it will require general anesthesia. This is because the skin in this area possesses a large number of sensory nerves (pain fibers) that would be triggered during cutting of the redundant skin; general anesthesia ensures that these pain fibers are shut down during the operation.
What should I expect after brachioplasty surgery?
You should expect to feel sore throughout the upper arm in the early postoperative period. The soreness can be minimized by continuous wearing of the compression garments. In general, the compression garments should be worn for at least 2 weeks in order to prevent development of any contour abnormalities. Lymphatic drainage compromise is most common in these areas. Lymphatic drainage is promoted by performing mechanical massage, body wraps, and external ultrasound treatments when needed.
When will I be able to return to work following brachioplasty surgery?
Patients can expect to return to work within 1 week to 2weeks following brachioplasty surgery. Patients are advised to gauge their return to work by their overall soreness which dictates the tasks which they may perform.
Are there any side effects associated with brachioplasty surgery?
Due to the extent of redundant skin excised, patients may experience increased tightness around the upper arms. This may lead to temporary swelling of the lower arms and hands.
Prolonged swelling up to 3 months is not uncommon due to poor lymphatic drainage following extreme weight gain and loss. Lymphatic drainage is further compounded by extended surgical incisions required to remove the redundant skin.
Lymphatic drainage is promoted by mechanical massage, body wraps, and external ultrasound treatments when necessary. Despite attempts to remove all redundant skin, patients may develop recurrent skin laxity following surgery, described as “Recurrent skin laxity Syndrome.”
This return of laxity is due to the loss of skin elasticity, a direct result of prolonged skin stretching throughout the years of obesity. Differences in laxity in local regions of the asymmetry may be responsible for slight asymmetry that develops following surgery.
Temporary numbness in the arms is possible as sensory nerves that are not visible to the eye may be transected by virtue of excising redundant skin.
Are there any risks associated with brachioplasty surgery?
Surgical treatment of brachioplasty patients requires specific precautions mainly because patients may be compromised physiologically but also because the surgeries can be quite extensive.
Patient safety is the most critical consideration when managing these patients whose hemodynamics and ionic balances may be altered. Patients are encouraged early ambulation in order to minimize the risk of developing vein clots which can then embolize (travel) to vital organs.
Intraoperatively, patients are also provided safeguards against vein clots with intermittent pneumatic compression boots and anti-thrombotic medication through the veins if patients still have a high BMI.
Another consideration involves correcting ionic imbalances resulting in iron deficiency anemia and B12/Folate deficiencies. Early blood work evaluation allows Dr. Paris to correct all abnormal parameters in preparation for surgery.
Other intraoperative measures include safeguarding against pressure sores with generous cushioning of the axilla (armpits), knees, heels, pelvis, and elbows.
Finally, patients with a larger ratio of surface area to volume are at risk for hypothermia (cooling of core body temperature) and should be provided a warm operating room, warming blankets, and warm fluids by vein. Surgical incision lines may present healing difficulties.
Wound breakdown is more common in these patients secondary to several metabolic and physiologic disorders. Diabetes and nutritional deficiencies are largely to blame for the difficult healing of these patients.
Seroma formation refers to the accumulation of plasma fluid in pockets created by the surgical elevation of the soft tissue. This fluid accumulates due to a low blood count and protein deficiency both of which are often present in post-bariatric patients. This fluid can be a nuisance to patients requiring several aspirations in the office prior to their resolution. More importantly, these plasma fluid pockets may harbor bacterial growth and result in a clinical infection. To counter the formation of seroma and to protect incision lines, customized compression garments are used to cover upper arm incisions.
Patient-Specific Questions:
Does everybody undergoing skin reduction surgery need to undergo brachioplasty surgery?
Patients who lose extensive weight will notice the deflation of their skin due to the loss of fat cell volume. The redundant skin can be quite extensive and may be aesthetically unsightly and functionally prohibitive.
When patients come for their consultation, it is fascinating how patients are unique and demonstrate weight gain and loss of the different regions. For example, one patient may have the most prominent skin redundancy isolated to the legs, another may demonstrate thin lower limbs and skin redundancy isolated to the arms. As such, not every post-bariatric patient may require brachioplasty.
Do patients need to be monitored by a nurse overnight following brachioplasty surgery?
Patients undergoing post-bariatric surgery are evaluated much in the same manner as other surgical patients. If patients have medical illnesses other than the redundant skin they are trying to eliminate, then they will require an overnight stay at one of the local overnight stay houses near our office or have a nurse accompany them at home.
In addition to identified medical illnesses, patients are evaluated with respect to their body mass index. The body mass index (BMI) is a parameter that measures the degree the patient is overweight. When the BMI is greater than 30, the patient is considered a high-risk candidate and recommended to spend the night with one of our registered nurses.
Overall, isolated brachioplasty procedure does not require overnight supervision; however, if multiple surgeries are performed such as in a total body lift, then overnight supervision with a nurse may be recommended.
Can you get arm numbness following brachioplasty surgery?
Arm numbness can occur if the antibrachial/median sensory branches are injured during surgery. Injury to these nerves is minimized by utilizing liposuction to hydrodissect the nerves away from the redundant skin planned to be excised.
What steps can be taken to minimize scarring of the arms?
The upper arm can be vulnerable to poor scarring following brachioplasty. As such, we utilize an aggressive scar prevention protocol.
This starts with minimizing the tension of the incision line with a multi, 3 layered closure of the incision line. In addition, specialized tapes, called Steri-Strips, are applied to the incision lines which act as an external stitch without the risk of railroad tracking.
Steri-strips are maintained for one month, after which, topical silicone tape and/or gel is recommended for another two months. During this recovery period, Intense Pulse Light therapy and steroid injections will be implemented when necessary.