
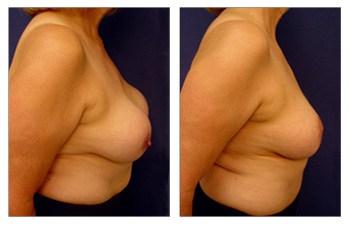
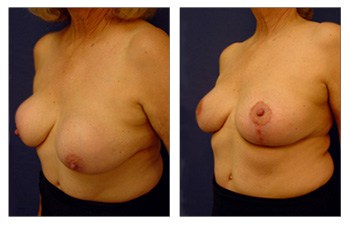

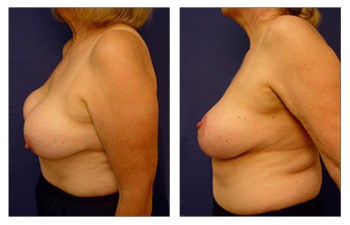
After having breast implants, some women experience capsular contracture. Capsular contracture is when your breast implant gets scarred up and firmed. Visually, a capsular contracture looks like a stuck in place breast implant and the breast mound sagging over it. It is possible to improve this with a Breast lift with implant augmentation to correct capsular contracture.
This is also what we call a snoopy deformity. When using silicone implants, the implant gets sticky and may result in this snoopy deformity. Just as a comparison, saline implants will move down with the breast mound and nipple-areolar.
Capsular contracture is corrected by a breast lift, and some patients take this opportunity to increase their implant size. When performing a breast lift with implant augmentation to correct capsular contracture, there are two different concepts to keep in mind.
a) The first concept relates to when and if the capsules aren’t super thickened. If the capsules are too thickened, as a surgeon, you can use the slightly thickened capsules to advantage when doing a breast lift with implant augmentation.
This can be an advantage to surgeons because, in a breast lift with implant augmentation to correct capsular contracture, you are having to reposition the implants and make room for a larger implant. If the capsules are not extremely thickened, we are able to preserve the blood flow better, manipulate the pocket malposition, and are still able to use the lateral or superior capsule to counter lateralization.
One example is if the breast lateralizes, you will see the breasts sagging off the chest as you lose the pectoralis area, creating a falling effect of the breasts to the armpit area. In a breast lift revision, or a breast lift with implant augmentation to correct capsular contracture, the goal is trying to centralize and medalize the breasts, sewing the pocket laterally.
Another example is when or if the implants sag with breast and areola, a capsulectomy will be done to create a new pocket on the chest wall. If the implants are stuck, there is a worry about the breasts being malpositioned or moving up. In these cases, we recommend the use of a breast band.
If you have silicone implants and the breast pockets are up high, this can be used strategically by the surgeon. This will keep the superior capsule in place, blocking the implant from going up, so no breast band is required. Another situation is when going bigger, the prior capsule needs to be released to make room, so a capsulorrhaphy, and sometimes capsulectomy is performed.
b) The second concept relates to when and if the capsules are very thickened, up to a point that does not allow the breasts to expand. In this case, your surgeon will have to remove the whole capsule. If this is the case, then why not remove the capsule all the time?
The answer is that a slightly hardened capsule often helps if the skin is thinned out, which can lead to the implant being exposed. A capsule preserves blood flow to the nipple and is vascular. If the capsule is able to be preserved, your surgeon will work to manipulate it, rather than remove it, as it is helpful to ensure blood flow to the nipple.
In general, when we use a vertical mastopexy, the main concern with a breast lift with implant augmentation is preserving that blood flow as there are back cuts that already compromise horizontal blood flow. Compressing the nipple-areolar can also compromise the perpendicular or vertical blood flow, so avoiding this risk by keeping the capsule is preferred.
Here we present our 58-year-old patient who demonstrates a breast lift with implant augmentation to correct capsular contracture. The patient previously had what is called snoopy deformity, where the implant sat high and the breast mound sagged below.

