WANT THE CONFIDENCE THAT COMES WITH
KNOWING YOU LOOK YOUR BEST?

Secondary Rhinoplasty CASE STUDIES

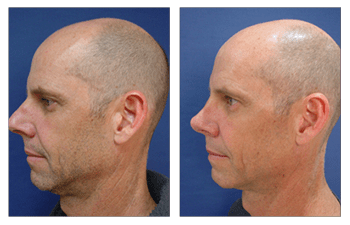
Secondary Rhinoplasty
Secondary rhinoplasty is indicated for patients who desire a revision rhinoplasty. Patients who had prior rhinoplasty are frequently referred to Dr. Paris for various reasons including nasal dorsum contour irregularities, suboptimal nasal tip shape or malpositioning and compromise of nasal structural support infrastructure leading to difficulty breathing.

Irregularities in nasal dorsum contour can result from withering nasal dorsal bony irregularities of the upper third of the nose or from poorly supported upper lateral cartilages which results in "an inverted V" deformity of the middle third of the nose.
Irregularity in nasal dorsal bony contour can arise either from prominent bony spicules that create compromise of the overlying nasal skin or from asymmetric infrastructure and medialization of the nasal bones causing a crooked nose deformity. Either deformity can be corrected by revising the previously performed osteotomies. The correction of the inverted V deformity requires reinforcement of the upper lateral cartilage to the dorsal septum utilizing a spreader graft.
The suboptimal nasal tip shape is characterized as an amorphous tip, in contrast to a refines nasal tip shape, and result from improperly performed nasal tip cartilage stitching (intradomal and interdomal stitches).
This deformity can be corrected by revising the nasal tip cartilage stitches and infrequently introducing Onlay cartilage grafts. Since only cartilage grafts are vulnerable to resulting in an operated look, Dr. Paris advocated softening all Onlay graft edges and camouflaging the grafts with a temporalis fascia.
Suboptimal nasal tip positioning is frequently observed and results from poorly reinforced nasal tip cartilage structures resulting in a tip that is lower than the nasal dorsum. When the nasal tip does not lead the nasal dorsum, the tip appears droopy as characterized by the parrot beak deformity. Correction of this deformity required reinforcement of the nasal tip cartilages as described in the "Nasal Tip Rhinoplasty" page.
Patients who develop difficulty breathing following rhinoplasty demonstrate constriction of their internal nares due to poorly supported upper lateral cartilage and nasal dorsal septum junction resulting in constriction (internal nasal valve constriction), concavity of the middle third nasal sidewall due to a weak upper lateral cartilage canopy, or from pinching of the nares entryway at the alar rim (external nasal valve constriction).
Correction of the internal nasal valve constriction requires the placement of spreader grafts. The collapse of the middle third nasal sidewall can be corrected with placement of alar batten grafts which are placed in the nasal sidewall and which stent up the middle nose soft tissue. Finally, the correction of a pinched external nasal valve requires placement of alar contour graft that is placed directly into the alar rim and helps stent open the entryway.
Frequently Asked Questions:
You should definitely wait six months for swelling to subside, otherwise you are operating on something that has not settled down and would be guessing as to the final results. It is ideal to wait one year so that you are assured not to have it move again.
Narrowed nostrils require alar rim contour grafts that can be done in the office and really not considered a formal closed or open rhinoplasty. Concern is that usually there is not enough cartilage following prirmary rhino in the septum; you may want to consider using your ear cartilage (conchal bowl). An alternative to the above, is to use a cadaveric cartilage graft.
I’m wondering if I would most likely get a surgery to my nose? Cosmetic or to fix the broken bone?
Patient-Specific Questions:
Unfortunately, trying to fix your nose surgically is only going to make it thinner. I would recommend using a filler to cushion your nasal cartilages and to help fix any irregularities. This is safe and some of the filling will create scar tissue which will make your nose look more bulbous as you desire.
If your columellar strut is too long, this is the only exception I would make to revising it using a closed approach; otherwise an open rhinoplasty provides more visualizatoin and more accurate adjustment.
You can't really reverse you rhinoplasty but you can have a revision rhinoplasty in order to get rid of the silicone (this is no longer the ideal dorsal onlay as it will eventually become unstable and fail) and to have it replaced with diced rib graft (remember that this can be obtained from an organ donor) as well as deprojecting your tip at the same time
Tip grafts using the closed approach is a crap shoot because you cannot see how the shape will look in its final position; with the closed you can deliver the tip out the side, change it, and then hope that it looks good when you pop it back. The open is the GOLD STANDARD for altering the tip.