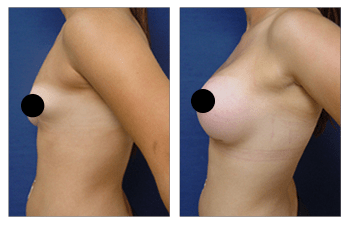

Correcting congenital breast deformity requires differential analysis and a customized surgical plan for each breast. This is because embryologically, each breast develops independently to the other. Thus, in a single patient, we will often observe and underdeveloped in one breast yet an overdeveloped breast in the other.
The underdeveloped breast often lacks both mound volume and demonstrates a herniated nipple and areola complex. This is because the underdeveloped breast mound is often contracted and does not allow the glandular tissue to grow out. Instead, the glandular tissue pushes out on the areola region causing it to herniate out despite a lack of mound volume.
Correcting congenital breast deformity in the underdeveloped breast requires placement of a breast implant. This maneuver will result in countering the breast mound contraction by augmenting the mound throughout. In addition, the dilated areola must be reduced in size in order to improve the overall breast to areola proportion and harmony.
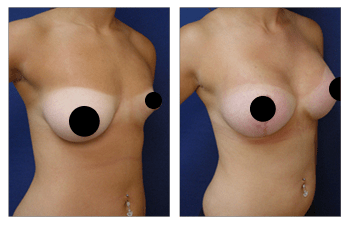
In contrast, the overdeveloped breast can demonstrate enlargement in volume and compensatory growth of skin that results in breast sagging. Correcting the breast deformity in the overdeveloped requires a breast lift with implant augmentation. The breast lift will eliminate the redundant skin as well as lift the nipple and areola complex to a more optimal position.
The addition of the implant will ensure appropriate breast mound roundness and fullness that is symmetrical with the implant augmented contralateral underdeveloped breast.
Correcting congenital breast deformity will result not only in physical improvement in breast appearance but also result in improved mental well being. Since congenital breast deformity changes become apparent as early as young teenage years, clients are often observed to develop insecurities as early as in their high school years.
This can result in inhibitions displayed in physical education classes. In later years, patients with congenital breast deformities may have a more difficult time with intimacy and developing relationships.
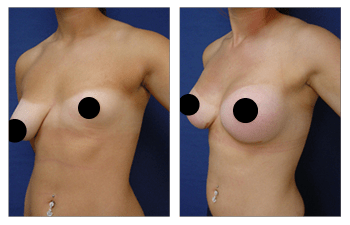
When correcting congenital breast deformity, your surgeon must be cognizant of each patient’s maturity level and comfort level with incision lines. Incision lines may result in temporary scarring that may be aesthetically unappealing to a younger patient. The need for prolonged surgical incision lines develops from the need to perform breast lifts as well as from the need to reduce areola sizes.
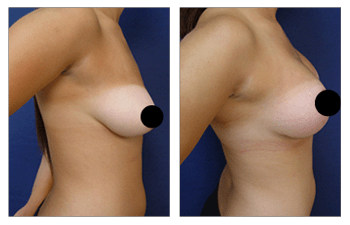
It is important to discuss the pros and cons of correcting congenital breast deformity. In general, even our younger patients have demonstrated satisfaction with gains achieved in overall breast contour and mound symmetry that have outweighed the need for surgical incision line placement.
The 18-year-old female patient demonstrated breast surgery to correct congenital breast deformity.

