Correcting breast asymmetry must consider both shape and size differences between the two breasts. Asymmetry may involve several factors relating to the nipple and areola complex as well as the breast mound. The nipple and areola complex may vary in size and shape as in position.
Often one nipple and areola may demonstrate moderate to severe sagging while the opposite nipple and areola are not sagging at all. Moreover, one breast may demonstrate a herniated areola complex that is enlarged in comparison to the other areola. This need correcting breast asymmetry.
The herniated areola is most often associated with the smaller breast that is underdeveloped during its embryologic phase with the resulting contraction of breast tissues. Since the breast tissues a tight, the growing glandular tissue will push out and herniate the areola.
The asymmetry of the breast mound is characterized by both variable size and position. Often one breast mound will develop more generously than the other breast. The more developed breast mound will typically be saggier in appearance. This is in contrast to the less developed breast that demonstrates no sagging at all.
Interestingly, breast size variability can be quite drastic between the two breasts. Correcting breast asymmetry typically requires a customized surgical plan that is dictated by the asymmetry demonstrated.
Correcting breast asymmetry requires a combination of variable breast implant size use to correct size discrepancies and simultaneous breast lift to correct nipple and areola position and size asymmetry. The breast lift will allow for lifting of the nipple and areola complexes to a more desirable and optimized position. The new implant position is determined by the choice of implant. This is because the implant must be centered on the new implant position.
This is why consideration of breast mound size variability is so important since the new nipple position will be dictated by the implant size and style chosen to correct breast mound size discrepancy. This is because the inframammary crease to nipple distance must equal the radius of the new implant.
Typically, the difference in implant size is minimal between the two sides, because most of the lower breast pole asymmetry can be corrected with the breast lift excisions.
When the chest is viewed it becomes that most asymmetry is in fact over the lower breast pole and that minimal asymmetry exists over the upper breast pole. Asymmetries over the upper breast pole are typically resulting from chest width variability that can be corrected using variable breast implant styles.
In correcting breast asymmetry, implant style differences, such as low, middle, versus high profile, provide your surgeon to use variable sizes in implants but still preserve identical implant radius to make sure that the breast volume discrepancies are corrected without creating different breast widths and upper pole fullness.
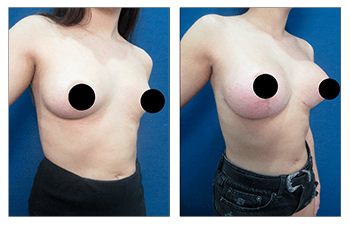
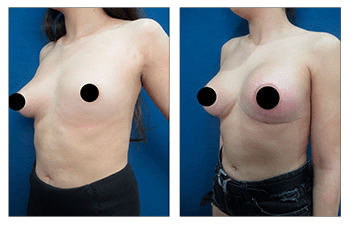
18-year-old female patient shows correcting breast asymmetry with left breast mound void that was 80% smaller than the right breast.

