


Breast reduction in general is performed to reduce the weight of breast tissues that can pull on your upper back and neck. However, these functional considerations should not neglect aesthetic priorities. As a result, breast reduction is achieved by utilizing optimal incision patterns that take into consideration each patient required breast tissue elimination needs.
As such, patients must undergo a comprehensive evaluation to determine where the breast fullness and drooping are located. The reduction is achieved then by customizing the incision lines to address all of the problem spots with regards to redundant skin as well as the breast prominences with regards to glandular tissues and fat.
The surgery requires the use of an incision pattern described as the Weiss pattern. The Weiss pattern utilizes incision lines that allow for the preservation of blood supply to the nipple and areola complex while allowing for removal of undesirable medial and lateral breast tissue excess.
The tissue excess that is undesirable is mostly located over the lateral breast areas and less over the medial breast. When breast reduction is performed appropriately, it should result in not only reduction of breast tissue and weight but also beautiful contour lines that are rounded in appearance and aesthetically pleasing. Best breast reduction surgery requires the creation of breasts that are both functionally improved with respect to the elimination of tension on your neck but also breasts that are youthful in appearance with respect to the appropriately positioned nipple and areolas as well as breast mound that are aesthetically pleasing visually.
If you are having upper back and neck pain because of your sagging and enlarged breasts and are considering a breast reduction surgery, we encourage you to take advantage of Our Surgical Team’s expertise so that you can get this procedure available.
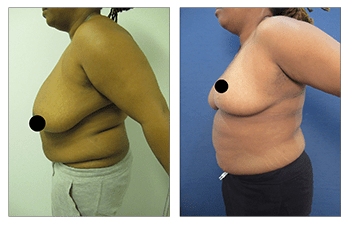
Please see a 35-year-old female patient who shows how best breast reduction can improve bilateral symptomatic breast hypertrophy and ptosis grade III.

